
Mentoplasty: isolated aesthetic chin surgery or in combination with orthognathic surgery
Traducción automática
El artículo original está escrito en idioma ES (enlace para leerlo) .
Introduction
The lower third of the face plays an important role in appearance and harmony. Disharmonies of the chin produce a disarray between the lower third and the rest of the face and have a relative impact on the attractiveness and harmony of the face. Changes with chin surgery in its position, proportion, and contour have a significant impact on the balance and harmony of the face.
Chin surgery will be addressed in this article as a means to restore harmony and restore the congruence of the lower part of the face. Genioplasty is an excellent complement to camouflage procedures in class II orthodontic treatment. Many patients seeking orthognathic surgery of the jaws and/or rhinoplasty also require alteration of the chin to achieve optimal balance of their face. Many patients are unaware of the importance of the chin in their profile and the influence it has on the soft tissues, especially the neck's double chin.
Genioplasty is especially used for the treatment of a chin that is poorly projected anteroposteriorly, but it is very useful for vertical alterations both decrease and increase and for slight asymmetries. Chin surgery is performed using prosthetics or through osteotomies. The sliding osteotomy is the procedure we use almost exclusively as it versatilely and predictably influences the soft tissues and the bony contour, achieving a more natural aesthetic profile with fewer complications.
Consultation-Evaluation-Preoperative
The first consultation for a patient affected by a chin alteration includes:
1. Complete medical history. 2. Complete dental history with special emphasis on orthodontic treatment. 3. Complete facial and dental photographs. 4. Lateral cephalometric radiograph. 5. Orthopantomography.
Functional and aesthetic objectives are determined according to physical examination and complementary tests. If there are associated dental or skeletal anomalies, plaster models will be taken. This information is used to advise the patient on surgical, orthodontic, or combined possibilities. Recommendations will be made taking into account dental or facial alterations and/or the severity of the deformity. Patients who only wish for cosmetic correction of the chin and do not want treatment or have been adequately orthodontically treated will also be explained.
Surgical technique
Bone genioplasty, although we have performed it under local anesthesia and intravenous sedation, is more comfortable and safer when performed under general anesthesia.
The vestibule and lower gingivolabial groove are infiltrated with a solution of 0.5% lidocaine or 1/100000 adrenaline along with infiltration of the suprahyoid muscles of the floor of the mouth.
The most comfortable position for the surgeon is at the head of the patient. The lip is retracted and a cut is made in the mucosa 5 mm below the mucogingival junction, leaving a rim of the chin muscles attached to the bone, from canine to canine. The periosteum is detached with an Obwegesser elevator without reaching the lower portion of the symphysis to avoid chin ptosis.
The exit of the vascular-nervous bundle is located more or less at the height of the first premolars. Only the mandibular bone below the foramen of the dental nerve will be periosteally detached. A 701 bur will mark the midline. With a reciprocating saw and under abundant irrigation, the cut will be made 4-5 mm below the exit of the nerve. We must remember that the nerve bundle has a lower path and then makes a loop upwards to exit through the mental foramen, which is why the horizontal cut should be positioned 4-5 mm below this.
The direction of the cutting line determines the alterations in the vertical dimension of the chin; the greater the angle between the occlusal plane, the more the chin will shorten. The surgeon must always ensure that the cut is complete at both lateral ends and at the lingual cortex to avoid irregularities when placing the osteomuscular flap and also to prevent the use of chisels that can even cause jaw fractures.
Case 1
Advancement mentoplasty without vertical change. The patient presents with dysfunction of the temporomandibular joint with pain, clicking, and limitation of mouth opening. The patient was treated with a relaxation splint, developing a severe class II malocclusion. The patient underwent surgical intervention after orthodontic preparation performed by Dr. Antonio Páez. A mandibular sagittal osteotomy was performed with an advancement of 7 mm and an advancement mentoplasty without vertical changes of 7 mm. The patient improved, with the joint pathology disappearing and achieving a satisfactory occlusal and aesthetic result.
If you want to considerably shorten the chin, an osteotomy will be performed, first making the caudal cut and then the cephalic cut, removing a wedge of bone. If we want to lengthen the chin, we use predetermined blocks of non-resorbable hydroxyapatite.
Before proceeding with the fixation of the osteomuscular segment, the genioglossus and suprahyoid muscles should be visualized and assessed for any bleeding vessel that could cause a hematoma in the floor of the mouth and coagulate it. It will also be checked if there is any palpable step at the lower mandibular end, and if so, it will be regularized. Almost always, we use plates for fixation, although 3 wires work very well except for vertical augmentations.
The closure of the incision is meticulous and is performed in 2 layers, first suturing the muscular layer and then the mucosal layer. Finally, a compressive dressing will be placed with horizontal tape over the labiomental groove and another vertical from the floor of the mouth and the lower mandibular ridge, which will be removed after 3 days. There are no dietary restrictions, and the patient will rinse with saline after eating for 10 days.
Case 2
Vertical augmentation mentoplasty. Patient affected by class II malocclusion and vertical and sagittal hypoprojection of the chin. The patient was treated with orthodontics by Dr. Daniel Díez and subsequently underwent sagittal mandibular osteotomy with an advancement of 8.5 mm and vertical augmentation mentoplasty of 7 mm and advancement of 3 mm. A non-resorbable hydroxyapatite block was used, which was rigidly fixed between the fragments of the chin osteotomy.

Case 3
Vertical reduction mentoplasty. Patient no. 3 is a patient with an open bite and class III malocclusion and a significant vertical excess of the chin. The patient was treated with Lefort I osteotomies, ramus osteotomies, and vertical shortening mentoplasty of 8 mm.
Case 4
Centering mentoplasty. The patient presents with severe mandibular hemielongation causing asymmetry and class III. The patient was treated with sagittal ramus osteotomies, and once an adequate occlusion was achieved, chin asymmetry persisted, leading to a centering chin osteotomy. Achieving almost perfect mandibular symmetry.
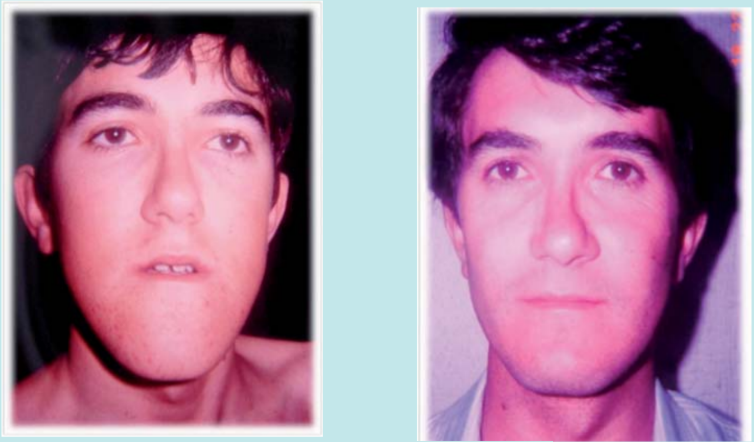
Case 5: Nasal aesthetic surgery and chin contour.
Cosmetic surgery. The 18-year-old patient presents with a severe nasal deformity and desires a strong mandibular contour. Septorhinoplasty was performed along with a 6 mm advancement mentoplasty.

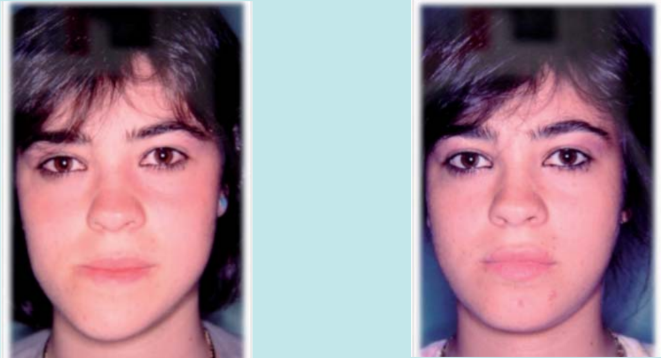
Case 6: Cosmetic nasal surgery and mentoplasty
Cosmetic surgery. The patient has completed orthodontic treatment and presents with moderate nasal deformity and a chin with sagittal and vertical hypoprojection. I performed septoplasty removing 2.5 mm of bony dorsum, 3 mm of cartilage, reduction of the cephalic edges of the alar cartilages, and osteotomies. The chin was vertically elongated by 4 mm and advanced by 4 mm, achieving harmonization of the entire face with a splendid aesthetic result in both frontal and profile views.

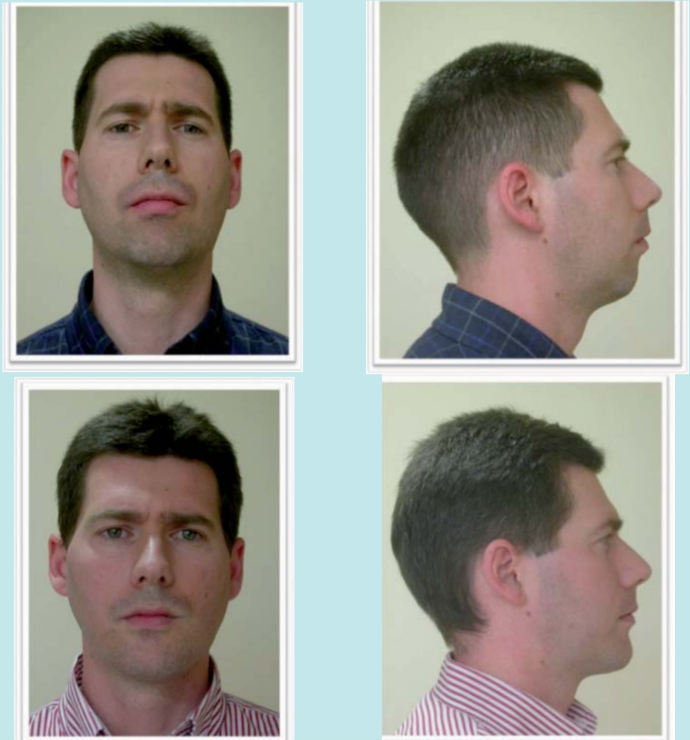
Case 7. Cosmetic nasal surgery plus advancement mentoplasty
The patient is finishing orthodontic treatment. Orthognathic surgery was not offered, and he comes for camouflage surgery. The patient presents with a severely hooked nose and hypoprojection of the nasal tip. He has a severe sagittal deficiency of the chin. The patient underwent surgery with septorhinoplasty, maintaining the masculine and ethnic characteristics of the patient, and an advancement mentoplasty of 8.5 mm. The aesthetic result is fabulous, achieving a harmonization of the profile and forehead, improving the double chin and resulting in an apparent rejuvenation.

César Colmenero, Javier Prieto Serrano, Fe Serrano Madrigal
Bibliography
- Sarver D. Esthetic orthodontics and orthognathic surgery. Ed Mosby 1998.
- Rosen HM. Aesthetic guidelines in genioplasty. Plast reconstruct surgery 1995: 95.
- Rosen HM. Surgical correction of the vertically deficient chin. Plast reconstruct surgery. 1988: 82.247-56.